Il s’agit du troisième site en France à proposer cette modalité thérapeutique, après les centres d’Orsay (Ile-de-France) et de Nice. Au regard de la rareté de ce type d’équipement sur le territoire national, le Centre François Baclesse propose cette option thérapeutique, en coordination avec les autres centres, à la population du territoire français, ainsi qu'à des patients venant de l’étranger.







Centre François Baclesse
Service de Radiothérapie
3 avenue Général Harris
14076 CAEN cedex 5
+33 (0)2 31 24 34 48

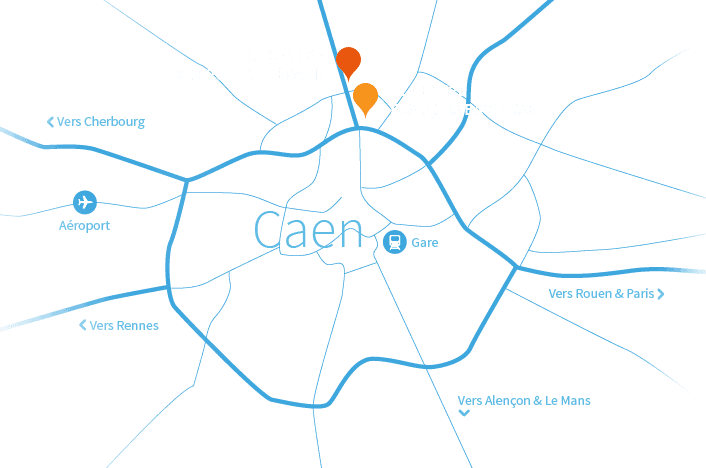
Centre de Protonthérapie Cyclhad
35 Allée de Dakar
14200 Hérouville-Saint-Clair